Palatal expansion was first described in1860 but didn’t come into widespread use in orthodontics until nearly 100 years later. Dr. Andrew Haas of Ohio was the most influential advocate of jaw expansion and used “rapid palatal expansion” in many of his treatments. Known for his non-extraction orthodontic approach in an era when extraction was coming to be done on many patients he influenced many orthodontists to use expanders and avoid extraction.
Underdevelopment of both jaws has become widespread in all industrialized societies as people adopted a Western Diet which requires little chewing force. Jaw expansion has become a response to this problem. Jaw expansion is possible because of the presence of a suture allowing the two halves of the upper jaw to move laterally. Expanders can be fixed (cemented on the teeth) or removable (attached to the teeth, but removable for activation and cleaning). There are advantages and disadvantages for each type.
Expanders were first used to correct posterior crossbites (narrowness of the upper jaw resulting in upper teeth being narrower than the lower teeth). Because the lower jaw has no midline suture orthodontists were universally afraid to try to expand the lower jaw. Most orthodontists confined use of orthodontic jaw expanders to the upper arch and achieved no more than 4-5 mm of expansion. In the mid-1980’s Dr. J. Michael Dierkes (then head of orthodontics at Emory University) presented a paper to a prestigious orthodontic group advocating simultaneous palatal expansion as well as expansion of the mandible (lower jaw).
When I heard Dr. Dierkes speak nearly 40 years ago, I began expanding both jaws for my own two boys. We call expansion of both jaws “Arch Development”. This became a crucial part of our practice in developing jaws to make more room for the teeth, the tongue, and improve the airway for our patients. Expansion of 10 mm or more is easily possible. My own grandson has had this very treatment just like we did for his father. Sadly, there are still many orthodontists who still are afraid to change and adopt this easy and effective treatment.
If you are an orthodontist, pediatric dentist, or general dentist doing orthodontics and getting into airway treatment here are some things you need to know about palatal expansion:
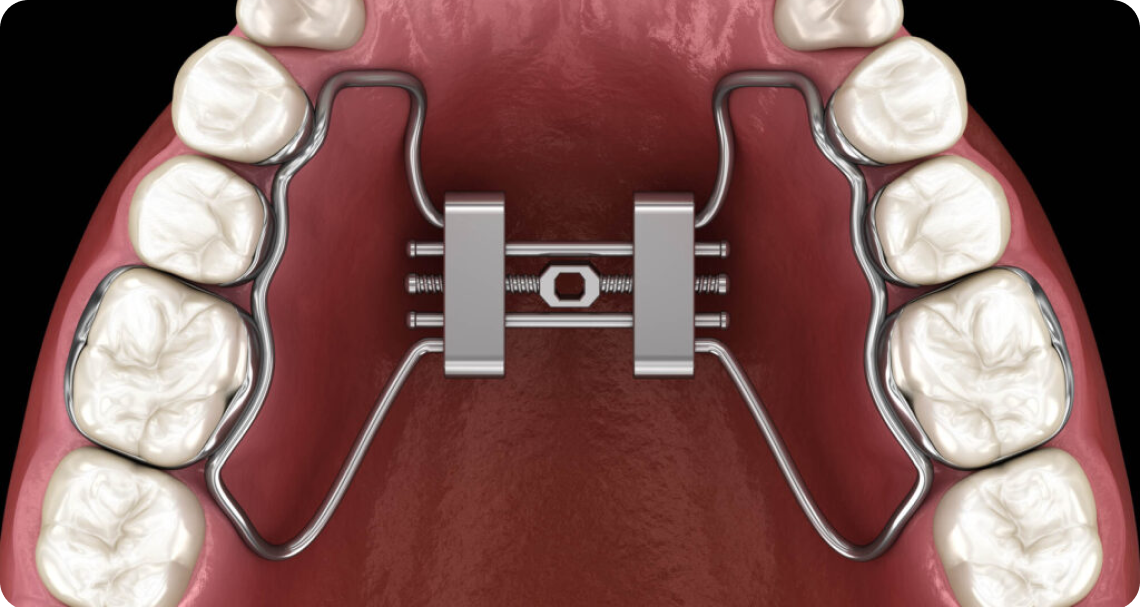
A palatal expander is a removable or fixed appliance which applies a force to laterally widen the upper jaw. It creates room for all the teeth to be aligned when they are crowded and can improve the airway.
Used under the direction of a well-trained dentist, palatal expanders are very safe and quite effective in correcting problems they are designed to correct. Learn more at OrthO2Health’s website!
If you’re a practitioner looking for more information about tongue ties and airway health, we offer courses and mentorship programs at Ortho2Health. Visit Ortho2Health to learn more and collaborate with experts.