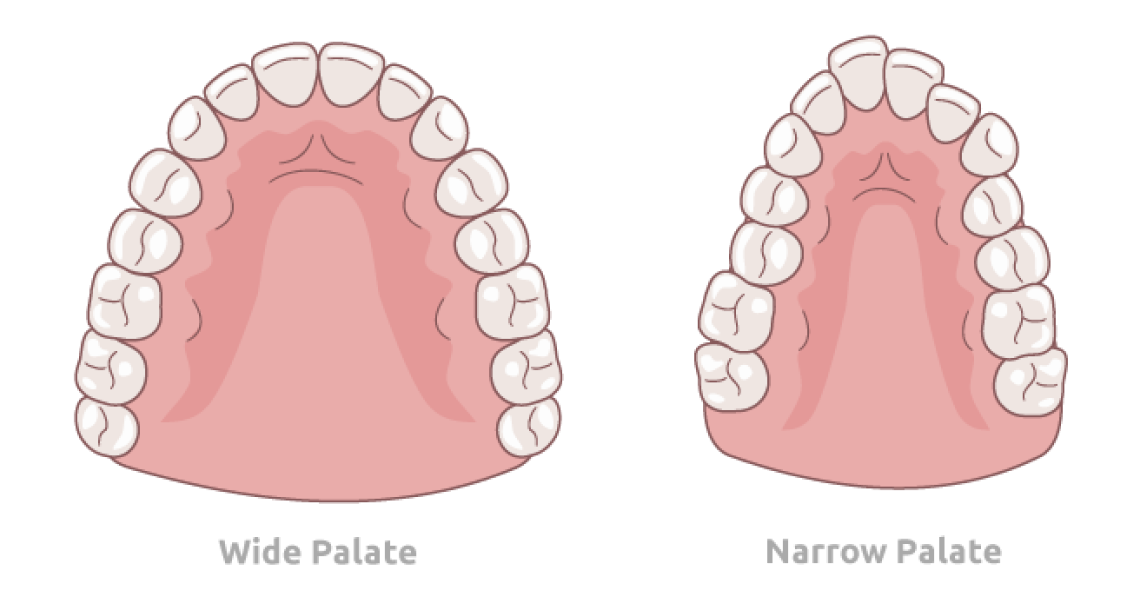
Narrow palates have become incredibly common, but we were all meant to have broad palates with enough room for our teeth. What happens to produce a narrow palate, and what are the possible impacts of this? We are genetically programmed to grow a wide palate, and we all would if we kept our teeth together, our tongues to the plate, and our lips together at rest. Many, if not most, children in modern industrialized societies hang their mouths open and have low rest tongue posture. The palatal width is determined by a balance between the tongue pushing laterally against the teeth and the cheeks pushing inward. With low rest tongue posture the cheeks are pushing in 100% of the time and the tongue is too low to counter that force. The cheeks win and the dental arches narrow.
If the dental arches are narrow the teeth have less bone to live in and they become crowded. When they erupt they lack space, and orthodontists have been trained that such crowding should require removal of teeth to avoid pushing the teeth “off the bone support” and “making a case more stable”. There is no support in the literature for either of these ideas but they persist. With teeth being removed, the space for the tongue gets even smaller and the poor rest oral posture gets worse. A narrow smile results which is always less esthetic than a broad smile. A narrow, unattractive smile is bad enough, but the health implications of a narrow palate are far more important. The tongue falls back in the throat and can easily compromise the airway leading to breathing disorders both night and day with OSA (Obstructive Sleep Apnea) a highly possible outcome.
Along with the narrowness of the palate in the lateral plane of space, the same low rest tongue posture and lack of contact of the teeth together at rest frequently produces a longer, more convex face with both jaws recessed in the face. A high narrow palate is associated with such long faces. When that occurs, the soft palate and the tongue move back even more and can produce an even worse breathing pattern with OSA ultimately being a highly likely outcome. Untreated OSA carries a penalty of a 20% reduction in life expectancy. Every chronic disease known to man is correlated to untreated OSA with heart attack, stroke, cancer, diabetes, Alzheimers, etc. all being more likely. Crooked teeth pale in importance to the incidence of these dreaded conditions.
Both upper and lower jaws were being expanded for medical reasons even in children under age 6 in the late 1800’s and early 1900’s. That practice fell out of favor and was replaced with adolescent orthodontic treatment in the mid 20th century. Braces were put on all the teeth when all permanent teeth were in the mouth with teeth frequently being removed. The focus became the teeth. The face and the airway implications were ignored. Thankfully, today some are focusing more on the face and airway with straight teeth being a nice side benefit.
We have been expanding BOTH the upper and lower arches since the mid-1980’s. Space CAN be made for all the teeth and extractions eliminated. The palate CAN be widened so that the tongue can properly fit there. This can be done for people of all ages.
Ideally we should get back to treating kids in the primary dentition before any permanent teeth erupt into crowded positions. More importantly, we need to improve the child’s rest oral posture to be nasal breathers with their tongues to the palate so they don’t develop narrow palates, and they can achieve forward growth of the face and optimized airways.
Curious to learn more about narrow palates and their impact on airway health? Visit Ortho2Health for in-depth resources, expert insights, and helpful information on how these issues can affect overall well-being.